Correcting the COVID Record, Part II - The Unnecessary Panic
Co-published on Odysee, Publish0x, and Zirkels.
In Part I, I looked into the masking data from the Cochrane Library. It turned out that using surgical masks did not improve health outcomes from respiratory viruses, including COVID. And while N-95 masks showed a larger effect, it was statistically insignificant. The chances that these were false negatives were low as the sample sizes were more than sufficiently large. This came in direct contradiction against what the mainstream media, medical establishment, and much of the governments swore by: that wearing masks would reduce the spread of COVID. They hardly did, if at all.
Going further into the COVID rabbit hole, I realized that the erroneous responses to the COVID outbreak back in 2020 were worse than I expected. I have already talked about Anthony Fauci's emails and the mainstream media's bizarre crusade against ivermectin, and those were bad. But as I read into this seroprevalence meta-analysis from Pezzullo et al. (2023), I asked myself how did this (the response to the outbreak) was botched so badly.
The Real Infection Fatality Rate
To set the context, the study analyzed 31 seroprevalence studies, all of which had sampling periods in 2020, in order to calculate the infection fatality rate (IFR). Some studies sampled early 2020; others collected data mid-year; and a few continued sampling into 2021. Knowing the history of the COVID variants, these studies observed the seroprevalence of the alpha and delta variants which were the deadliest.
In addition, the patients in each of the studies did not receive the Pfizer, Moderna, or any of the other COVID injections. In addition, the studies did not include patients who had prior infections to COVID. To get straight to the point of this specific tidbit, Pezzullo et al.'s (2023) effectively calculated the IFR of patients who had no prior immunity to the virus. As a result, we're theoretically looking at the worst of the worst situation.
The results showed a median infection fatality rate (IFR) for 0-59 yo of 0.034% and an IFR for 0-69 yo of 0.097%. When analyzing by country, Italy had the highest IFR of 0-59 yo at just a little above 0.13%. If you expand the scope to 0-69 yo, the IFR goes up for all countries. But even then, the highest IFR is a 0.35% (again from Italy).


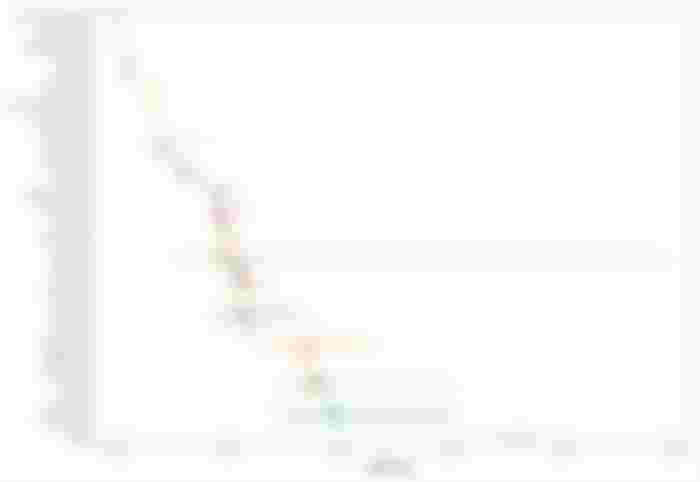

The results make sense when you think about it. COVID is more dangerous to the elderly population than the younger demographics. Italy has the highest IFR while it has the lowest proportion of the population below 60 or 70. I wished the study performed an age-adjusted analysis, i.e. pretend that the population distribution of all countries are the same. But if Italy had the same distribution as a nation like Israel, then it would have a smaller IFR.

The biggest story, in my opinion, is when the IFR is stratified by age. We know that the general IFR is extremely low and COVID disproportionately affects the elderly population. So how much lower is the IFR when we look at children, teenagers, and young adults? Well here's the data in boxplot form:
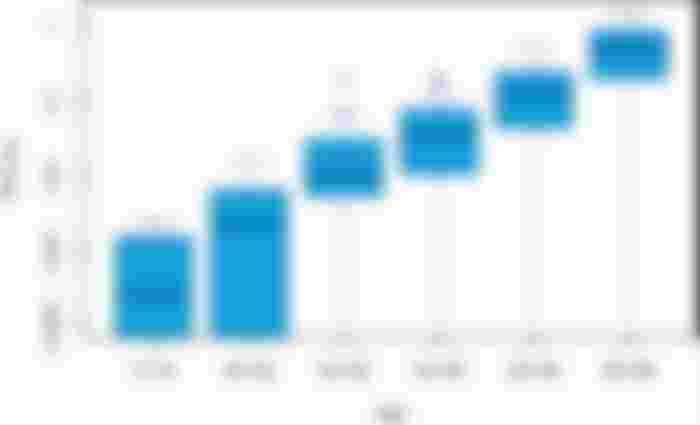
Patients aged 0-19 had an IFR of a measly 0.0003%; 20-29 yo had an IFR of 0.002%; 30-39 yo clocked at 0.011%; 40-49 yo had an IFR of 0.35%. It's not until you go past 50 yo when the IFR finally exceeds 0.1% at 0.123%. Lastly, 60-69 yo had an IFR of 0.506% which is still not even a full single percent. Looking more closely, when you go up an age cohort, the IFR approximately quintuples. You can infer the IFR for people over 70 by multiplying the IFR of the 60-69 cohort by five and you will get around 2.5%.
Closing Thoughts: The Unnecessary Overreaction
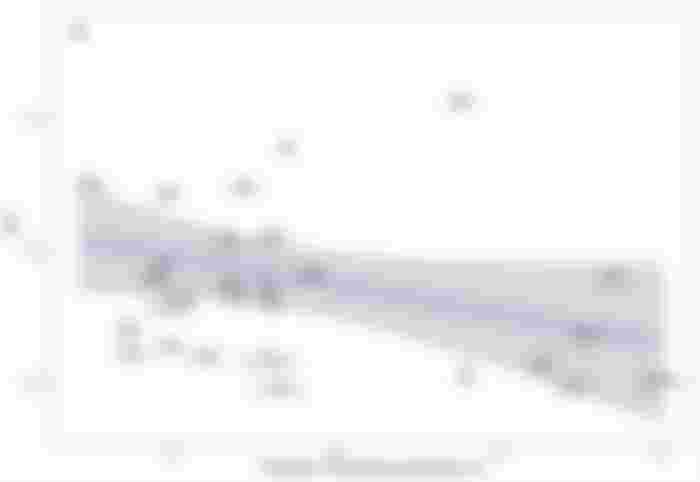
When putting all the pieces together, even in the worst case scenario, the infection fatality rate could not clock over 1% unless we specifically look at people over 70. There's a clear correlation between the IFR and the median age of a population. When I look back at the lockdowns, the mandates, and penalties governments imposed on their citizens, I cannot help but ask "What the fuck were they doing?".
Many small businesses were forced to shut down while the big box retailers were allowed to remain open. Many of the mom-and-pop shops shuttered permanently. Children and teenagers exhibited learning deficits when schools shifted to virtual learning. Those who tried to defy the lockdowns and mandates were fined and arrested. All this to combat a virus that had an extremely low IFR (and the lockdowns proved to be useless, too, as demonstrated by a Johns Hopkins University study I wrote about months prior).
It also puts into perspective the vaccine mandates. Politicians tried to mandate students from kindergarten to high school to take the COVID injections even though the IFR of their age group is not even a thousandth of a percent. The same applied to universities that made students get vaccinated or else they could not take classes. However, the injections did not prevent the spread of COVID, so the idea of vaccinating the young demographics to protect the elderly was moot. Instead, what should have been done was to boost the immunity of the vulnerable >70 population and have the resources ready for them in case things go south. Oh, and not stuffing COVID-infected patients in nursing homes would've made a difference, too.
Who knows how much of this debacle is attributable to incompetence and malice. Regardless, this is something that must never happen again. Such heavy-handed measures to a rapidly spreading pathogen likely caused more pain and suffering than the pathogen itself.
Stay tuned for Part III.