Not medical, legal, or any other advice - reported for information only.
The US Centers for Disease Control and Prevention (CDC) are observing cases of heart inflammation - myocarditis and pericarditis - in young recipients of the mRNA vaccines since April 2021. While public health officials and "TV doctors" are minimizing this risk by labeling vaccine-induced myocarditis as "mild", independent MDs suggest that there is no such thing as a "mild" heart inflammation. Indeed, the National Institutes of Health's introduction to the topic, linked from the above CDC page, characterizes the condition as "causing damage" (presented as a certainty, not a possibility), which "can lead to serious health problems" and may require "medicine, procedures, or possibly surgery" as well as lead to complications up to "heart failure".
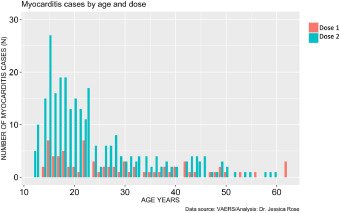
An article titled "A Report on Myocarditis Adverse Events in the U.S. Vaccine Adverse Events Reporting System (VAERS) in Association with COVID-19 Injectable Biological Products" by Canadian microbiologist Dr. Jessica Rose and well-known American cardiologist and COVID critic Dr. Peter McCullough finds a high rate of myocarditis in males age 13-23. For the younger range of these ages, the authors statistically confirm that the incidences of adverse-event reports of myocarditis is far above the normal rate in the population and much greater after receiving the second dose of a COVID-19 vaccine. The article was accepted for publication in the journal Current Problems in Cardiology after peer review. However, after being published on 1 October 2021 with status "online ahead of print", it was temporarily withdrawn two weeks later, with an apology from the publisher currently replacing the text of the article. The original text is still available via the Internet Archive's wayback machine.


The VAERS data studied by Rose & McCullough are often criticized for the voluntary and non-authoritative nature of the submitted reports. Yet, VAERS is the official pharmacovigilance system in the US. In fact, the Federal Drug Agency's (FDA) approval letter for the Pfizer vaccine, requires the manufacturer to monitor adverse events. The approval unambiguously links to "guidance [that] provides information and recommendations pertaining to the electronic submission of postmarketing safety reports involving vaccine products, including individual case safety reports (ICSRs) and attachments to ICSRs (ICSR attachments), into the Vaccine Adverse Event Reporting System (VAERS). VAERS is a national vaccine safety surveillance program ..., which requires health professionals and vaccine manufacturers to report specific adverse events that occur after the administration of routinely recommended vaccines." (emphases added by this author).
To paraphrase the FDA guidance on adverse events, reports are required for all health issues arising after someone receives a vaccine. It is not a necessary to be certain that the issue was caused by the shot. Instead, the combination of all suspected cases submitted to the system will be used for the detection of "safety signals". That is, public health administration is supposed to look for clusters of type, frequency, or severity of adverse events that suggest the need for further examination. And this has happened with the COVID vaccines. For example, when the AstraZeneca product was first associated with blood clots, and "out of an abundance of caution", the province of Ontario stopped using it for first doses on 11 May 2021. Note that the safety signal in this case, the incidence of "vaccine-induced immune thrombotic thrombocytopenia" suspected to be caused by the AstraZeneca vaccine, had reached 1 in 59,000 (1.7 in 100,000).


On 24 March 2021, Health Canada required the addition of a warning to AstraZeneca's product monograph. Only five days later, Canada's National Advisory Committee on Immunization recommended to pause the product in people under 55, and Canada eventually donated over 750,000 doses of the shunned concoction to countries in central and south America.
Back to myocarditis, my home province detected another safety signal when the rate of heart inflammation in young males reached 1 in 5,000 with the Moderna vaccine, almost twelve times the risk of blood clots when the AstraZeneca product was stopped. On 29 September 2021, Ontario's medical officer of health recommended the Pfizer/BioNTech product over Moderna for individuals aged 18-24, since the myocarditis occurrence with the Pfizer shot was estimated at "only" 1 in 28,000 (still twice as high as our comparator safety signal!). Again, this step was taken "out of an abundance of caution".


Fast forward two weeks when Public Health Ontario reported on "Adverse Events Following Immunization (AEFIs) for COVID-19 in Ontario: December 13, 2020 to October 10, 2021". Myocarditis is discussed as an "adverse event of special interest". Table A3, hidden in the appendix of the 26-page report, displays a host of rates per million by age group, gender, and dose. Upon closer inspection, some rates stand out as much higher than the average or typical rates: those for males in the three youngest age groups, between 12 and 29 years, in particular those after dose 2. As often, a graphical presentation of the same data (columns females dose 1 & 2 and males dose 1 & 2 only) makes the outliers stand out more clearly.


If those tall bars don't present a safety signal, than what does? Note that the magnitude of the highest reporting rates of 120 and 173 per million is eerily similar to the rates of 162 and 94 per million in younger and older teenagers, as reported in a controversial preprint posted 8 September 2021. That study by Høeg et al. famously estimated the risk of cardiac adverse event as up to six times higher than the risk of being hospitalized for COVID-19 itself. Based on the Ontario government data discussed here, it would appear that Høeg et al. discovered the safety signal in US some six weeks ago. Taking their findings seriously could have prevented harm in children.


And indeed, if we utilize the Internet Archive again to retrieve older versions of the Public Health Ontario report, we find that the myocarditis incidence in young males, including children age 12-17, has kept growing over the last couple of two-week periods between 11 September 2021 and 10 October 2021. With expanding vaccination mandates, e.g. for children's sports, we continue to "spread" vaccine injuries in our most precious generation.
Nice to meet someone who is similar to me regarding back up your statements with facts. Yet those who follow blindly will make an excuse that all your evidence provided here "its worth the risk" until 5 years down the line when the true effects are known. Even the UK is making excuses now that vaccine immunity is short lived and that's why they have so many cases. What they fail to state is that they're going into their winter and people have gotten really unhealthy through lockdowns. They also like to leave out how many people died of flu every year before the "pandemic".
Anyway, excellent articles. I like reading your posts with the data sources!